

This is Your Heart on Menopause
A woman's heart disease risk is different. Here's how to understand what happens to your heart health.


The menopause transition, a.k.a. perimenopause, influences the chances for cardiovascular issues, which includes heart disease, stroke, and high blood pressure, and not in a good way. Since cardiovascular disease (CVD) is the leading cause of death in women living in the U.S., it’s worth exploring your risk in midlife and beyond, which includes your pregnancy experiences.
Higher Blood Lipids
Though aging is a factor for CVD, research shows that menopause plays a significant role. Estrogen helps shield women from heart disease and other cardiovascular conditions, including high blood pressure and stroke. Estrogen loss, a hallmark of menopause, strips away that protection.
A study published in the American Journal of Epidemiology illustrates what happens to blood lipids, such as the different types of cholesterol, when estrogen declines. For seven years, researchers followed nearly 2,700 pre- or perimenopausal women as part of the Study of Women’s Health Across the Nation (SWAN). On the whole, total cholesterol, low density lipoproteins (LDL), and apolipoprotein B, a compound that ferries LDL around the body, increased significantly starting the year before a woman’s final menstrual period (FMP) and lasting through the year after the FMP. Some experts think that apolipoprotein B is better than cholesterol for determining risk. A normal apolipoprotein B level for women is 60 to 117 mg/dL.
The postmenopausal women in the study had more than double the chance for elevated LDL than the premenopausal participants. In spite of their name, LDL contain high cholesterol concentrations. Excess LDL increase the risk for heart disease by contributing to fatty plaque build-up that blocks the flow of blood to the heart, brain, and legs.
In the same SWAN study, high density lipoprotein cholesterol (HDL) also peaked in late peri- and early postmenopause. High-density lipoproteins are often called “good” cholesterol because of their relatively low levels of cholesterol, and because they can remove cholesterol from cells involved in plaque build-up in arteries. The thinking is that higher HDLs help protect against heart attack and stroke, but that may not be the case after menopause. There is some evidence that HDLs don’t function in the same beneficial way with estrogen loss and that higher levels of HDL may actually promote clogged arteries.
Triglycerides are another name for fat. Elevated triglyceride concentrations in the blood contribute to clogged arteries, but triglycerides are not directly affected by the menopause transition. Triglycerides are sensitive to diet and lifestyle, however. Excess added sugar, fat, and alcohol can increase blood triglyceride levels, while omega-3 fats, such as the kind found in fish, help lower them. Having overweight or being sedentary may also result in higher blood triglycerides.
Here are the goals for the most common lipid blood tests.
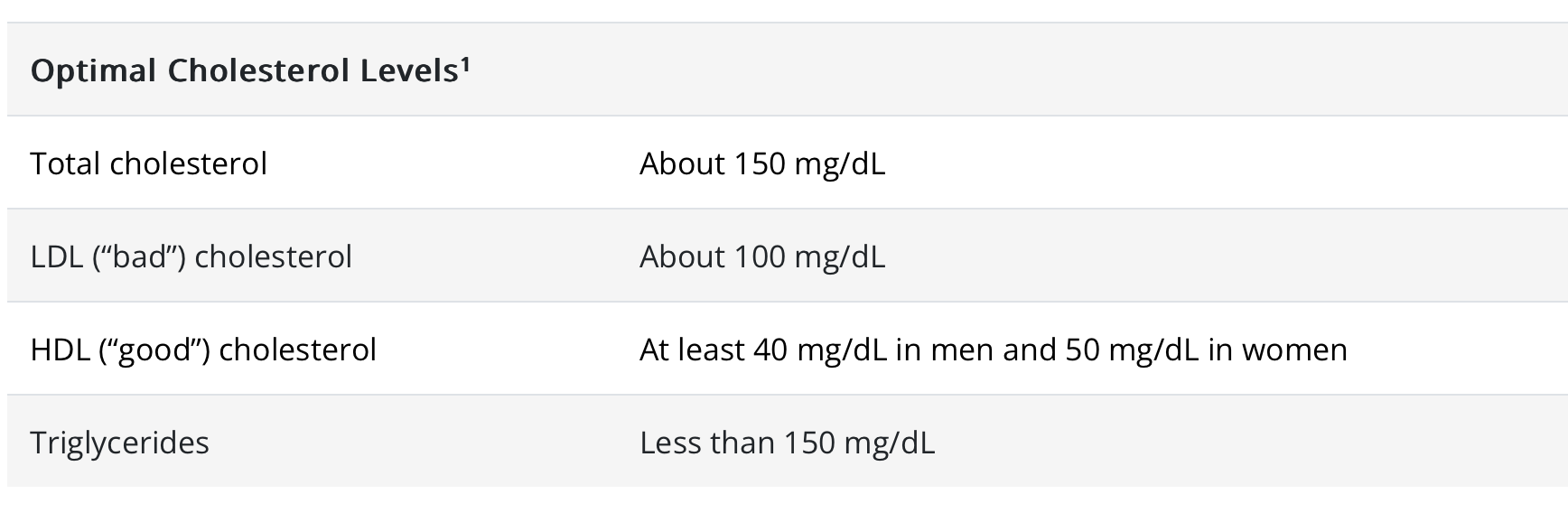
Source: https://www.cdc.gov/cholesterol/about.htm
There is another component of your blood that you should check on, especially if your LDL is elevated. It’s called Lp(a) and it’s a type of LDL. High levels of lipoprotein Lp(a) increase your likelihood for heart attack, stroke, and aortic stenosis by increasing inflammation and clotting in blood vessels.
High Lp(a) levels run in families, and are more prevalent in black people. A recent study in Maturitas pooled the results of 17 studies that examined the effect of estrogen loss on Lp(a) levels and the findings were inconclusive. Though Lp(a) is not routinely included when measuring other lipids, ask your health care provider to order it separately.
A desirable Lp(a) level is 50 mg/dL or less (or 125 nmol/L or less). Elevated levels of Lp(a) are not sensitive to diet, exercise, and other lifestyle habits, but can be treated with lipoprotein apheresis, a process that removes Lp(a) and from the blood.
Stiffer Arteries
Joints and muscles can get stiffer with menopause, and arteries can, too.
A study published in Arteriosclerosis, Thrombosis, and Vascular Biology found a significant increase in artery stiffness within a year of a woman’s FMP, and concluded that the stiffness was independent of aging and other risk factors. The researchers also found that black women may experience more arterial stiffness starting early in the menopause transition than white women.
Stiffer arteries are considered a marker for CVD and are one of the reasons why blood pressure increases with age. Menopause can contribute to arterial stiffness. Estrogen reduces inflammation in blood vessels, promotes blood flow, and supports a lower blood pressure.
Here are the goals for blood pressure.

Source: https://www.cdc.gov/bloodpressure/facts.htm
Body Composition
Excess body fat is linked to higher blood pressure, insulin resistance, elevated lipids, and inflammation, which all contribute to CVD.
On its own, menopause is not responsible for weight gain in midlife. (Don’t come at me – it’s science!) However, menopause may result in excess fat in the abdomen. Most of this fat is the visceral type, which differs from the subcutaneous fat on your thighs and buttocks. Visceral fat lies under the abdominal wall and its proximity to your internal organs is problematic. So is the fact that visceral fat produces more inflammatory compounds than the subcutaneous kind. According to the American Heart Association, visceral fat boosts CVD risk, regardless of your weight.
Having obesity can also contribute to a condition called coronary microvascular disease (MVD), which affects the tiny coronary artery blood vessels that branch off from the larger vessels near your heart. With coronary MVD, blood vessels aren’t clogged, but they are damaged in a way that results in decreased blood flow to the heart. Women have more MVD than men and lower estrogen levels increases the risk. Having high blood pressure before menopause, especially high systolic blood pressure (the top number), also heightens the chances for MVD.
There is a strong link between weight gain, and a higher midlife weight, and developing atrial fibrillation later on. Atrial fibrillation is an irregular heartbeat that can lead to blood clots, stroke, heart failure, and other heart problems. According to the American Heart Association, having obesity may be the cause of as many as 20% atrial fibrillation cases.
Blood Glucose Levels
Before menopause, women tend to have better insulin sensitivity and lower chance for type 2 diabetes compared to men of the same age, suggesting that estrogen is advantageous in keeping blood glucose and insulin levels within a normal range. As estrogen levels decline, it becomes harder to maintain normal glucose levels, which has implications for heart health. That’s because elevated glucose levels can damage blood vessels, making them more prone to fatty plaque development. A normal blood glucose is 99 mg/dL or less in a fasted state.
Skeletal Muscle Mass
About 30% to 40% of the body is skeletal muscle, the kind that’s connected to your bones. Skeletal mass allows you to move, protects joints by holding them in place. It’s also a metabolic machine that supports heart health.
Muscle supports normal blood glucose levels which helps to prevent insulin resistance, a condition linked to type 2 diabetes, high blood pressure, and clogged arteries.
You lose muscle mass with age, and menopause exacerbates the decline in muscle health. Regular exercise preserves and improves muscle health, and provides other cardiovascular benefits, including blood pressure management, lower blood glucose levels, and less inflammation.
Pregnancy and Heart Health
Pregnancy is a test of the cardiovascular system, and we’re learning more about how complications during pregnancy affect a woman’s future risk for CVD. Having one or more pregnancy complications is a heads up for managing your health going forward.

Hypertensive disorders in pregnancy (HDP), which include high blood pressure and preeclampsia, affect nearly 10% of pregnancies. A Journal of the American Medical Association Network Open study found that HDP are linked to a higher risk for heart disease and stroke in women years after delivery. A 2018 Hypertension study of women ages 41 to 58 who had a HDP found that the prevalence of high blood pressure, higher blood lipids, and type 2 diabetes was significantly greater than in women who never experienced a HDP.
Gestational diabetes presents another risk for CVD. One British Medical Journal article pooled the results of 20 studies and concluded that gestational diabetes increased the chances of developing type 2 diabetes by 10-fold compared to not having it.
Pregnancy loss also influences the chances for CVD. In a study of the relationship between miscarriage and cardiovascular health study published in the British Journal of Obstetrics and Gynecology, women who had experienced three or more early miscarriages (before the twelfth week of pregnancy) had a greater chance for developing high blood pressure and type 2 diabetes later on compared to women who never had a miscarriage. Research shows that type 2 diabetes and high blood pressure are also more common in women who experienced stillbirth, the loss of a pregnancy after 20 weeks. In addition, giving birth to a preterm baby is also a red flag for heart issues.
Take Charge of Your Heart Health
You can’t change your past lifestyle, pregnancy experiences, or your menopausal status, but you can try to control your future. Here’s how.
Know your numbers. Track your lipids, fasting blood glucose, blood pressure, and weight (if it’s not triggering for you) to help determine what steps to take to improve your health. Get a yearly physical and ask for a blood test that includes these values.
Advocate for the help you deserve. You are the sum of your experiences, and your doctor or nurse practitioner should consider the whole picture when assessing your health. Tell them about any complications you had during pregnancy, even if they don’t ask about it. It’s more likely for health care professionals to ask about a family history of heart attack or stroke or if you smoke cigarettes than it is for them to query you about your pregnancy experiences. Health care professionals need to know everything about you to formulate a plan for your health.
Follow a balanced diet. An eating plan rich in fiber that’s largely based on plant foods and low in saturated fat, sodium, and added sugar is the best strategy for cardiovascular health, and for your overall wellbeing, including weight control. A plant-based diet is not necessarily a vegan one devoid of animal foods. Lean and low-fat animal foods, such as milk, Greek yogurt, seafood, lean beef, and poultry, have a place in a heart-healthy diet. If you need help putting together a more plant-based diet, check out The Menopause Diet Plan, a book I wrote with fellow dietitian Hillary Wright.
Exercise. A combination of resistance training and aerobic activities is best. Experts suggest at least 150 minutes of moderate- to vigorous-activity, such as brisk walking, jogging, or biking weekly, which amounts to at least 30 minutes on most days of the week. They also recommend at least two weekly sessions of resistance training, such as weightlifting, that work all the large muscle groups. Resistance training is necessary for building muscle and preventing muscle loss.
If you smoke, quit. Smoking is linked to cardiovascular disease. Cigarette smokers are up to four times more likely to get heart disease than nonsmokers, and cigarette smoke doubles your risk for having a stroke.
Questions? Let me know in the comments!
Thank you for the article. Is the greater than/equal correct in this sentence: A desirable Lp(a) level is ≥50 mg/dL (or ≥125 nmol/L).
This post is great! I'll be making good use of the studies cited for a presentation on menopause I'm doing in a couple of months. Very concise and clear overview!